|
| Prenatal visit |
“The feature-length documentary BIRTH STORY: INA MAY
GASKIN & THE FARM MIDWIVES tells the story of counterculture heroine
Ina May Gaskin and her spirited friends, who began delivering each
other’s babies in 1970, on a caravan of hippie school buses, headed to a
patch of rural Tennessee land. With Ina May as their leader, the women
taught themselves midwifery from the ground up, and, with their
families, founded an entirely communal, agricultural society called The
Farm. They grew their own food, built their own houses, published their
own books, and, as word of their social experiment spread, created a
model of care for women and babies that changed a generation’s approach
to childbirth.
Forty years ago Ina May led the charge away from isolated hospital
birthing rooms, where husbands were not allowed and mandatory forceps
deliveries were the norm. Today, as nearly one third of all US babies
are born via C-section, she fights to preserve her community’s hard-won
knowledge. With incredible access to the midwives’ archival video
collection, the film not only captures the unique sisterhood at The Farm
Clinic–from its heyday into the present–but shows childbirth the way
most people have never seen it–unadorned, unabashed, and awe-inspiring.”
I really enjoyed
Birth Story.
It skillfully weaves together vintage footage, commentary, and births
with a present day shadowing of Ina May in her natural environment: at
the Farm. The documentary shows her working in her kitchen, eating,
talking to her husband, watering plants, riding her bicycle, teaching
workshops, training midwives, going to prenatal visits, and finally,
attending a very hands-off gentle waterbirth. It also lets us peek at
images from the early days of The Farm community, the caravan of buses,
the dreams of Stephen Gaskin and the “hippies” who followed him to
Tennessee.
Birth Story is
not just a film about Ina May though, it chronicles the experiences of
several other Farm midwives as well, and I loved hearing the commentary
and opinions of the less-famous midwives who helped transform the birth
world.
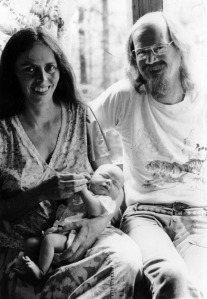
I found footage of Ina May with Stephen to be particularly poignant
and very much enjoyed the vintage photos and footage. I also find it
interesting how The Farm began because of Stephen’s leadership and ideas
and yet Ina May took off as the ongoing famous person in the family. Of
Stephen, Ina May explains: “He thought women we supposed to be
uppity—this was great relief, I didn’t like being held down.”
Ina May describes her own first birth explaining that in typical
birth climates, “there’s nothing about the special energy of birth and
that’s kind of the most important thing…I felt like I was doing
something sacred.” She also makes the basic and crucial point that the
number one rule of maternity care should be
Be Nice and
laughs as she asks us to consider how just those two words could change
maternity wards. There are only a handful of actual births in the film,
three of which are from sometime in the 1980′s. We see a breech birth
(a lot more hands-on than I think of present-day midwifery practice) and
a shoulder dystocia, both rare occurrences in birth films. We also see
brief footage of Ina May’s Safe Motherhood quilt project and a brief
discussion of disparities in maternal mortality rates.

Another highlight of the film for me was midwife Pamela, whose birth
we also see on-screen. She is shown telling us about an early birth she
attended saying, “I fell in love with women. How can you see someone be
so strong and not fall in love?” Exactly. My doula and friend, Summer,
who watched the film with me, developed her reaction to this quote in a
lovely blog post and it reminds me of my own past post about my own former midwife who helped me see that
midwife means loves women.
Ina May explains that she learned how to be a midwife by allowing
herself to be instructed by the women themselves and then she trained
other midwives. As I watched
Birth Story I found myself feeling a little sad, nostalgic, and bittersweet,
because I feel like the world that these beautiful midwives envisioned
has yet to really be birthed and that in some ways we’ve gotten so far
away from the relationship-oriented and community living/engagement
model upon which The Farm was based.
My initial feeling as I watched the film was that it would be
primarily of interest to people already very familiar with Ina May,
thinking that it may not appeal to or interest “regular” people.
However, the friends I viewed the film with had totally different
perspectives. One friend told me she thought her husband would really
have liked the documentary, particularly for the emphasis on community.
The one husband who was present reported that he thought everyone should
see the film and not just people who are already “birth junkies.” So, I
stand corrected, and will now say that
Birth Story has the capacity to engage with many people!
In 2007, I had the opportunity to listen to Ina May speak in person
at the La Leche League International conference in Chicago. She talked
about sphincter law and made the association with our bodies’ capacity
for bowel movements and women’s physical capacity to rebound from
childbirth. I will never forget her saying:
“I don’t know about you, but my butt closes back up after I poop.” That summed her up for me: plainspoken, real, matter-of-fact, and practical. She’s a legend!
 |
| Starstruck? Oh, yes I am. My husband said, “these people are like your *celebrities.*" |
–
Disclosure: I received a complimentary screening copy of the film for review purposes.